
Growth Hormone Peptides
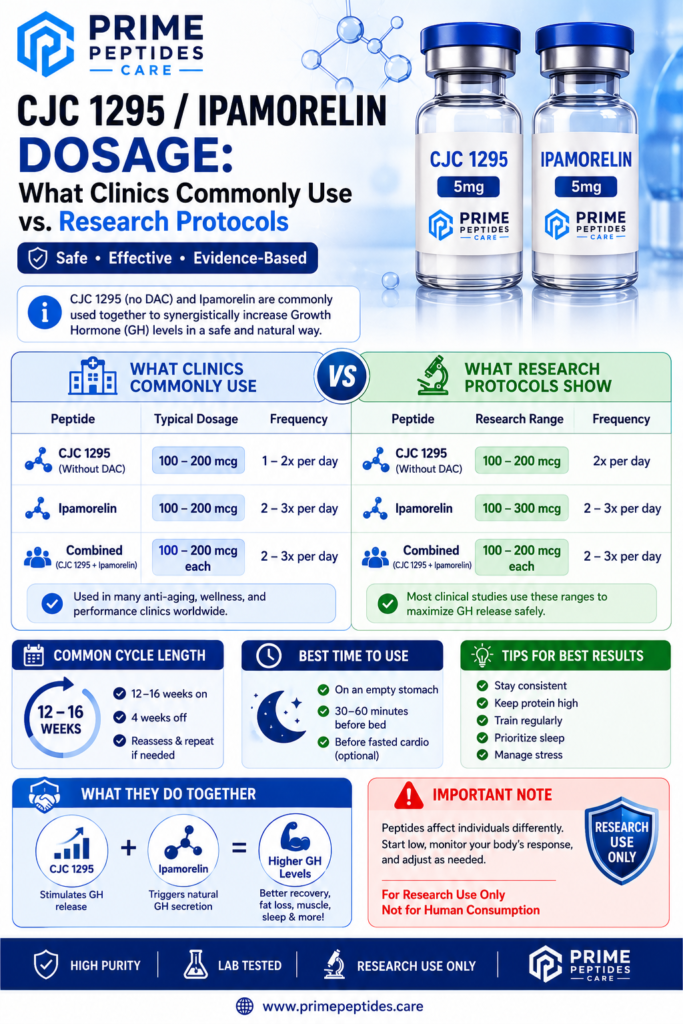
CJC 1295 / Ipamorelin Dosage: What Clinics Commonly Use vs. Research Protocols
May
Why dosage information matters
CJC 1295 and Ipamorelin are among the most talked‑about growth hormone related peptides online. Many people search for dosage information, but there is an important distinction between what medical clinics use under supervision and what researchers do in controlled lab experiments. This guide explains that difference in clear language and keeps everything framed as education not medical advice or instructions.
What are CJC 1295 and Ipamorelin?
CJC 1295 is a growth hormone releasing hormone (GHRH) analog.
It signals the pituitary gland to release more of the body’s own growth hormone over time.
Ipamorelin is a growth hormone secretagogue.
It mimics ghrelin at specific receptors and helps trigger short, sharp pulses of growth hormone.
When combined, clinics and researchers like this pair because CJC 1295 provides a longer baseline effect, while Ipamorelin creates quick pulses. Together they support a more “physiological” pulse pattern than constant stimulation.
How clinics typically approach CJC 1295 / Ipamorelin dosage
Real-world clinics that legally prescribe these peptides do not use one single fixed dose for everyone. Instead, they usually:
- Start with a low daily dose, often in the 100–200 microgram (mcg) range per peptide
- Give the blend as a subcutaneous injection, once per day, very often at night
- Adjust the dose upward slowly based on lab work, goals, and patient response
- Run time‑limited cycles (for example, several months on, followed by a break)
Key clinic patterns you see again and again:
- “Start low, go slow” – to watch for side effects and tolerance
- Night dosing on an empty stomach – to align with natural growth hormone pulses
- Medical monitoring – blood work, symptom tracking, and safety checks
Important: these protocols exist only in a clinical setting with licensed professionals. They are not meant to be copied at home and should not be treated as personal dosing instructions.
How research protocols differ from clinical dosing
In research environments, CJC 1295 / Ipamorelin use follows a very different logic:
- Everything is predefined in a protocol
Researchers write a detailed protocol before any experiment.
It specifies dose levels, timing, route of administration, animal model or cell line, and all measurement points. - Doses are often expressed per body weight
Instead of “X mcg per day,” research might describe dosage as “Y micrograms per kilogram” or similar.
This makes it easier to compare across different subjects or species. - Control and placebo groups are standard
A typical GH‑axis experiment includes:- A control group receiving no peptide or a placebo
- One or more groups receiving different doses of the CJC 1295 / Ipamorelin blend
This helps separate real peptide effects from background noise.
- Outcome measures are clearly defined
Research focuses on measurable endpoints, such as:- Growth hormone and IGF‑1 levels
- Changes in body composition
- Recovery markers
- Molecular signaling changes in specific tissues
- Everything is “Research Use Only” (RUO)
In lab protocols, CJC 1295 / Ipamorelin and similar blends are treated purely as research chemicals.
They are not used as medicines and are not administered to humans outside a regulated, approved environment.
Clinic protocols vs. research protocols: key differences
To keep this clear, here’s a simple comparison in words:
- Goal
- Clinics: symptom relief, performance, body composition changes under medical care
- Research: understanding mechanisms, pathways, and dose response relationships
- Who is supervised
- Clinics: individual patients under a licensed practitioner
- Research: animal models, cell cultures, or strictly controlled study participants
- Flexibility
- Clinics: doses may change visit by visit
- Research: doses are fixed by protocol; any change requires formal amendment
- Documentation
- Clinics: patient charts and follow‑up notes
- Research: lab notebooks, ethics approvals, statistical plans, and publications
Because of these differences, “clinic dosage” articles you see online are not the same as research protocols, even when they use similar numbers. On a research‑focused site like Prime Peptides Care, it is important to keep the emphasis on experimental design and RUO status.
Why you should not self‑dose based on online information
Many blogs and videos speak confidently about “the best” dosage for CJC 1295 / Ipamorelin.
However:
- Individual health conditions, medications, and lab values matter
- Growth hormone–related pathways can affect many organs, not just muscle or fat
- Only a qualified, licensed provider can decide if a GH‑related peptide is appropriate in a medical context
For that reason, any dosage information you see online including this article must be treated as educational, not prescriptive. If someone is interested in therapeutic use, they should speak directly with a medical professional who can order lab tests, review history, and provide individualized advice.
How Prime Peptides Care fits into this picture
Prime Peptides Care focuses on supplying high‑purity peptides labeled for in‑vitro research use only.
That means:
- Products are intended for laboratory experiments, not human or veterinary use
- They are not medicines, supplements, or cosmetics
- Researchers are responsible for complying with all relevant regulations and institutional guidelines
When your blog explains dosage concepts, always connect back to:
- Proper storage and handling
- The importance of clear written protocols
- The value of third‑party testing and certificates of analysis
- The RUO designation and legal boundaries
Key takeaways
- CJC 1295 and Ipamorelin work together by combining long‑acting GHRH‑like signaling with short pulses of secretagogue activity.
- Clinics typically use small, nightly doses under medical supervision and adjust based on labs and progress.
- Research protocols focus on predefined doses, control groups, and measurable endpoints, all within strict RUO frameworks.
- Online dosage information is educational only and should never replace professional medical advice.